

Abstract
Relapse of malignancy and lethal graft versus host disease (GVHD) are the principal causes of failure of allogeneic hematopoietic cell transplant (HCT). Recently we have shown that at seven days after HCT an algorithm using two serum biomarkers (ST2 and REG3α) can predict severe GVHD (Hartwell et al. JCI Insight 2017). We determined whether serial testing (in the first month following HCT) of patients with low probability biomarkers would improve the predictive accuracy of the algorithm and identify patients with different risks of relapse and lethal GVHD. Patients who received an HCT at 18 centers in the Mount Sinai Acute GVHD International Consortium (MAGIC) for hematologic malignancy and who supplied three blood samples were divided into a training set and validation set with equal numbers of lethal GVHD events, which was defined as death from GVHD or infection during treatment for GVHD. Patients in the training set (n=702) underwent HCT from January 1, 2006 until June 30, 2015, whereas patients in the validation set (n=906) underwent HCT from July 1, 2015 to May 1, 2017. Serum samples were analyzed using the previously published algorithm of two biomarkers up to three times (day 7, day 14, day 28 or GVHD onset, if onset occurred within the first 28 days). The algorithm generates a predicted probability of lethal GVHD between 0 and 1 for each patient. Patients were categorized as either low probability (LP) or high probability (HP) for lethal GVHD. HP thresholds of 0.20 and 0.16 were used to classify patients with and without GVHD symptoms, respectively (once categorized as HP, patients remained in that category and were not retested). All results were similar between training and validation sets, and we present here the validation set results.
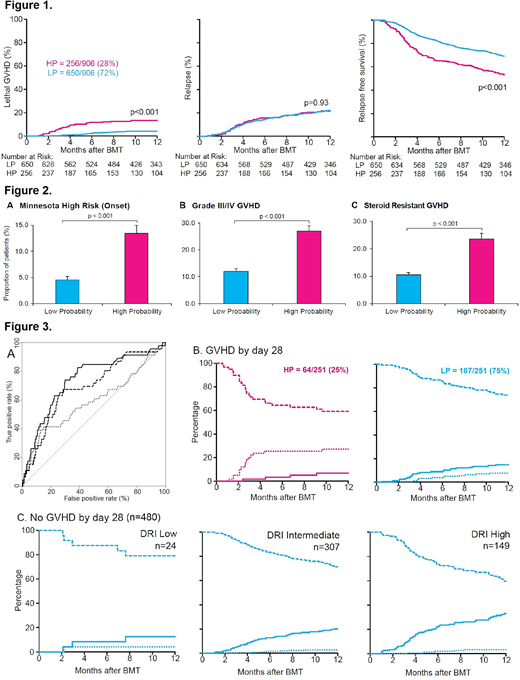
Serial testing identified 28% of patients as HP with a three-fold greater cumulative incidence of lethal GVHD at one year (13% vs 4%, p<0.001, Figure 1). Relapse rates were the same in both probability groups, and thus LP patients experienced significantly better relapse free survival (RFS) (69% vs 53%, p<0.001). As expected, significantly fewer LP patients experienced severe GVHD at onset (as measured by Minnesota risk), maximum grade III/IV GVHD, or steroid resistant GVHD by day 180 after HCT (Figure 2, p<0.001 for all three parameters). To measure the accuracy of prediction, at each timepoint we calculated the area under the curve (AUC) of receiver operating characteristic curves; the AUC increased significantly with each subsequent evaluation, from 0.59 at one timepoint (dotted line) to 0.74 at the third timepoint (solid line) (p<0.001), with a final sensitivity of 65% and specificity of 74% (Figure 3A).
Early development of GVHD (by day 28) is a risk factor for lethal GVHD. Therefore, we next plotted RFS (dashed line), relapse (solid line), and lethal GVHD (dotted line) rates in patients who developed GVHD by day 28. 25% of patients with GVHD were categorized as HP and had a cumulative incidence of lethal GVHD more than four times higher (28%) than that of relapse (6%); however the risks were reversed for the 75% of patients who were LP, where relapse (15%) occurred twice as often as lethal GVHD (7%) (Figure 3B). In patients who did not develop GVHD in the first month, this reversal of risks was even more dramatic. Approximately half (53%) of the entire validation cohort did not develop GVHD by day 28 and was LP at all three evaluations. These patients had an exceptionally low risk of lethal GVHD and thus they relapsed (25%) much more often than they died from GVHD (3%). When malignancies were classified according to risk for relapse by the disease risk index (DRI) (Figure 3C), the probability of relapse was three fold higher than lethal GVHD in malignancies with a low DRI (12%), six fold higher for intermediate DRI (20%), and eleven fold higher for high/very high DRI (33%).
We conclude that a serial monitoring strategy using GVHD biomarkers for one month after HCT is able to identify two groups of patients with very different risks of lethal GVHD and relapse. For these patients, the intensity of immunosuppression after day 28 could be tailored according to the probabilities of developing lethal GVHD and relapse in the context of clinical trials.
Aziz:Doris Duke Charitable Foundation: Research Funding. Ayuk:Therakos (Mallinckrodt): Honoraria; Novartis: Honoraria; Celgene: Consultancy; Gilead: Consultancy. Chen:REGiMMUNE: Consultancy; Incyte: Consultancy, Membership on an entity's Board of Directors or advisory committees; Magenta Therapeutics: Consultancy; Takeda Pharmaceuticals: Consultancy. Merli:Neovii Biotech: Honoraria; AMGEN: Honoraria. Roesler:Sanofi: Other: Travel, Accommodations, Expenses; Amgen: Equity Ownership; Jazz Pharmaceuticals: Other: Travel, Accommodations, Expenses; Immunomedics: Equity Ownership; Biogen: Equity Ownership; Merck: Consultancy; Pfizer: Consultancy. Kitko:Novartis: Consultancy, Honoraria; Mallinckrodt: Honoraria, Other: Travel, Accommodations, Expenses. Qayed:Novartis: Consultancy. Wölfl:Bristol-myers Squibb: Equity Ownership; Novartis: Equity Ownership; Taheda: Equity Ownership; Juno: Equity Ownership; Neovii: Other: Travel, Accommodations, Expenses. Mielke:Celgene: Speakers Bureau; DGHO: Speakers Bureau; EHA: Speakers Bureau; Kiadis Pharma: Speakers Bureau; Miltenyi: Speakers Bureau. Wudhikarn:Takeda Oncology: Other: Travel, Accommodations, Expenses. Nakamura:Celgene: Honoraria; Molmed: Honoraria; Merck: Consultancy; Pharmacyclics: Consultancy; Atara: Consultancy; Jazz Pharmaceuticals: Consultancy. Pulsipher:CSL Behring: Consultancy; Novartis: Consultancy, Honoraria, Speakers Bureau; Adaptive Biotech: Consultancy, Research Funding; Amgen: Honoraria. Reshef:Pfizer: Consultancy; Atara Biotherapeutics: Consultancy; Kite Pharma: Consultancy; Takeda Pharmaceuticals: Consultancy; Bristol-Myers Squibb: Consultancy; Incyte: Consultancy. Levine:Therakos: Consultancy; Novartis: Consultancy; Bluebird: Consultancy; Incyte: Consultancy; Kamada: Research Funding; Viracor: Patents & Royalties. Ferrara:Incyte: Consultancy, Honoraria, Other: Travel, Accommodations, Expenses; Xenikos: Consultancy, Other: Travel, Accommodations, Expenses; Kamada: Consultancy, Research Funding; Viracor: Consultancy, Patents & Royalties.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal